⚕️ Educational content only. This article explains sickle cell disease from a haematology and molecular science perspective. It is not medical advice. Consult a healthcare professional for personal health concerns.
Sickle cell disease (SCD) is a group of inherited haemoglobin disorders caused by a mutation in the HBB gene encoding the beta-globin chain of haemoglobin. It is one of the most common serious monogenic diseases worldwide and a key topic in haematology, molecular genetics, and global health. Understanding its molecular basis, laboratory features, and diagnostic approach is central to biomedical science education.
Key Takeaways
- SCD is caused by a point mutation in HBB (Glu6Val), substituting glutamic acid for valine at position 6 of the beta-globin chain.
- HbS polymerises under low oxygen tension, causing red cells to sickle, increasing haemolysis and vaso-occlusion.
- Laboratory diagnosis uses HPLC and haemoglobin electrophoresis to identify HbS and other variant haemoglobins.
- The blood film shows sickle cells, target cells, Howell-Jolly bodies (functional asplenia), and polychromasia.
The Molecular Basis of Sickle Cell Disease
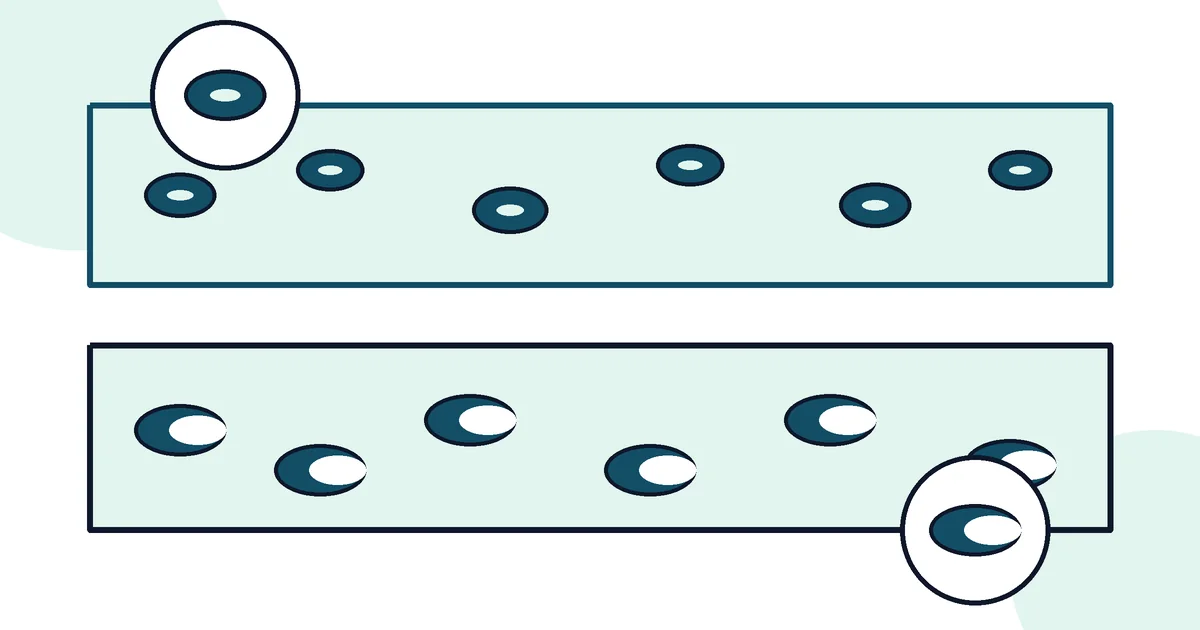
The cause of SCD is a single nucleotide substitution in codon 6 of the HBB gene: adenine is replaced by thymine (GAG → GTG), resulting in valine replacing glutamic acid at position 6 of the beta-globin chain (Glu6Val). The resulting abnormal haemoglobin is called HbS. Under deoxygenated conditions, HbS molecules polymerise into long fibrous chains that distort red blood cells into a characteristic sickle or crescent shape. These rigid, deformed cells cause vascular occlusion, haemolysis, and end-organ damage.
Inheritance and Genotypes
SCD follows autosomal recessive inheritance. The most common and severe form is HbSS (homozygous — both beta-globin alleles are HbS). Other clinically significant compound heterozygous forms include HbSC (one HbS allele, one HbC allele — HbC results from Glu6Lys mutation) and HbS/β-thalassaemia (one HbS allele, one thalassaemia allele). Sickle cell trait (HbAS) — one normal HbA allele, one HbS allele — is generally asymptomatic under normal conditions, though there are clinical considerations under extreme physiological stress.
Laboratory Diagnosis
HPLC (High-Performance Liquid Chromatography) is the first-line method for neonatal screening and diagnostic haemoglobinopathy testing in many countries. It separates haemoglobin variants by charge and retention time, identifying HbA, HbS, HbC, HbF, and other variants quantitatively. Haemoglobin electrophoresis (cellulose acetate at alkaline pH or isoelectric focusing) separates variants by charge under an electric field. Abnormal variants must be confirmed with a second method at different pH because some variants co-migrate. Sickling test (sodium metabisulphite) causes deoxygenation — sickle cells observed under microscopy confirm the presence of HbS, though this does not distinguish HbSS from HbAS or HbSC.
Blood Film Findings
The peripheral blood film in HbSS shows: sickle cells (elongated, crescent-shaped cells with pointed ends); target cells (bull’s-eye appearance, due to excess membrane); polychromasia (blue-tinged reticulocytes, reflecting increased erythropoiesis); Howell-Jolly bodies (nuclear remnants in red cells, a sign of functional hyposplenism/asplenia caused by repeated splenic infarction); and nucleated red blood cells in severe disease. The reticulocyte count is typically elevated (5–15%) reflecting compensatory erythropoiesis.
Full Blood Count Findings
Typical FBC in HbSS: haemoglobin 60–90 g/L (normochromic normocytic anaemia); MCV usually normal unless co-existing thalassaemia or iron deficiency; elevated WCC (neutrophilia, often baseline due to chronic inflammation); thrombocytosis (reactive, from functional asplenia); elevated reticulocytes. HbSC tends to have higher haemoglobin (90–110 g/L) and a milder clinical course than HbSS.
References
- WHO. Sickle-cell disease and other haemoglobin disorders. who.int
- NHS. Sickle cell disease. nhs.uk
- Rees DC, Williams TN, Gladwin MT. Sickle-cell disease. Lancet. 2010;376(9757):2018-2031.