After a nurse or phlebotomist draws your blood, you might wonder where it goes and what actually happens before a result appears on your patient record or GP’s screen. The journey from blood draw to reported result involves several carefully controlled steps, each designed to protect sample quality and patient safety.
Educational note: This article explains laboratory processes for educational purposes only. It is not medical advice and should not be used to interpret personal test results or make health decisions.
Key takeaways
- Blood samples go through three phases in the laboratory: pre-analytical, analytical, and post-analytical.
- Correct patient identification and tube type are critical before the sample even leaves the collection point.
- Specimen reception checks and registers every sample; the process is called accessioning.
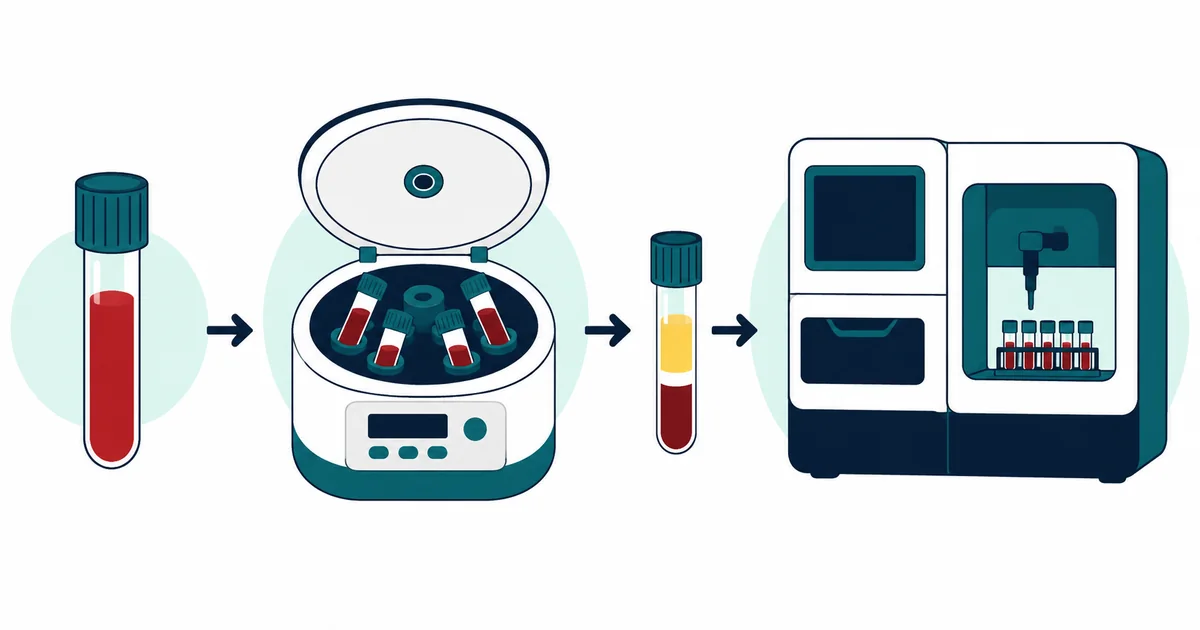
- Centrifugation separates blood into components; which component is tested depends on the test ordered.
- Results are validated by a biomedical scientist before being released to the clinician.
From blood draw to labeled tube
Collection starts at the bedside, clinic, or GP surgery. A phlebotomist or nurse draws blood into one or more colour-coded plastic tubes. The colours matter: each tube cap colour corresponds to a specific additive inside the tube. A purple or lavender cap contains EDTA, which prevents blood from clotting and is used for haematology tests including the full blood count (FBC). A gold or yellow cap contains a clot activator and gel separator, used for most biochemistry tests. A blue cap contains sodium citrate, used for coagulation tests.
At the time of collection, the tube must be labelled with the patient’s full name, date of birth, and a unique identifier such as an NHS number or hospital number. This label is the patient’s identity attached to the sample. Any mismatch, illegible label, or missing label means the sample cannot be safely processed.
Why patient ID and tube type matter
Patient identification is the single most important safety step in the entire process. A sample processed under the wrong patient’s name can lead to a result being matched to the wrong person, which can result in incorrect treatment decisions. For this reason, specimen labelling is governed by strict protocols in every NHS trust and accredited laboratory. Two patient identifiers are always required at a minimum.
Tube type matters because different additives affect different tests in different ways. Using the wrong tube can destroy red blood cells (haemolysis), prevent clotting when clotting needs to be measured, or introduce substances that interfere with analysis. Some tests require a specific minimum blood volume; underfilling a coagulation tube, for example, changes the ratio of blood to citrate anticoagulant and produces inaccurate results.
Transport to the laboratory
Once collected and labelled, samples are transported to the laboratory. In hospital settings, this may happen via pneumatic tube systems (vacuum-driven transport systems built into the hospital infrastructure), courier, or porter. GP and community samples are collected and transported by courier services, sometimes refrigerated for temperature-sensitive tests.
Temperature and time in transit matter. Some tests — particularly blood gases, certain hormones, and some haematology parameters — degrade if a sample sits too long before processing. Time stamps from collection through to receipt and analysis are tracked as part of quality management.
What specimen reception and accessioning do
When samples arrive at the laboratory, they enter specimen reception. This is where the pre-analytical process formally begins. Trained staff check every sample against a list of acceptance criteria. A sample may be rejected at this point if it is unlabelled, leaking, badly haemolysed (broken red blood cells, visible as a pink or red tinge in a serum sample), clotted when it should not be, or filled to an incorrect volume.
Accepted samples are “accessioned”: registered onto the laboratory information management system (LIMS) with a unique barcode. From this point, the barcode tracks every step the sample takes through the lab. Automation in modern laboratories means that a barcode scanner can direct a tube to the correct processing path without manual sorting in many cases.
Pre-analytical processing
Pre-analytical processing refers to everything that happens to a sample before it reaches the analyser. This phase accounts for the majority of laboratory errors in healthcare; estimates suggest 60 to 70% of laboratory errors originate in the pre-analytical phase, most of them outside the laboratory itself (during collection, transport, or labelling).
Sorting
On arrival, tubes are sorted by type and urgency. Urgent samples — marked STAT (from the Latin statim, meaning “immediately”) — are prioritised for faster processing. Routine samples are batched and processed in order. In highly automated laboratories, robotic sample sorters perform this task; in smaller labs, it is done by hand.
Centrifugation
Most biochemistry samples require centrifugation before analysis. Tubes are placed in a centrifuge and spun at high speed for a set time. The spinning force separates the blood by density. Red blood cells, being the densest, fall to the bottom. Platelets and white blood cells form a thin layer above them (the buffy coat). The liquid component rises to the top.
For gold-top tubes that contain a gel separator, the gel forms a physical barrier between the cellular layer and the liquid layer, making it easy to pipette off the liquid for analysis. Centrifugation settings — speed, time, and temperature — are standardised and validated to ensure consistent results.
Serum, plasma, and whole blood
After centrifugation, the liquid component is either serum or plasma, depending on the tube type.
Serum is the liquid remaining after blood has been allowed to clot and the clot and cells removed. It does not contain clotting factors. Most biochemistry tests — liver function, kidney function, cholesterol, HbA1c — are performed on serum.
Plasma is the liquid component of blood that still contains clotting factors, obtained from tubes with anticoagulant additives. Coagulation tests, and some specialist biochemistry tests, use plasma.
Whole blood (not centrifuged) is used for haematology tests, including the full blood count, where the cellular components themselves are what is being measured.
Analysis on lab instruments
Once prepared, the sample is loaded onto an analyser. In large NHS laboratories, many analysers are connected by automated track systems: robotic conveyor belts that move tubes from one instrument to the next without human handling. A blood sample may pass through a haematology analyser, a biochemistry analyser, and a coagulation analyser, all on a single automated track, with the LIMS directing each step.
Analysers work using various scientific principles depending on what is being measured: light scattering and electrical impedance for blood cell counting, spectrophotometry for enzyme activity measurements, immunoassay for hormones and proteins, and mass spectrometry for drug levels and complex molecules. Each method has been validated to ensure accuracy and precision within defined limits.
Quality checks and result validation
Automated results do not go directly to the clinician. Every result passes through a validation step. Instruments run internal quality control (IQC) samples alongside patient samples throughout the day. These are samples with known target values. If the QC result falls outside the accepted range, the batch of patient results may be held and the instrument recalibrated or investigated before release.
Biomedical scientists also review individual patient results. Computerised rules may flag a result as unusual if it is outside the reference range, significantly different from the patient’s previous result (a delta check), or inconsistent with other results from the same sample. A biomedical scientist then reviews the flag and decides whether to authorise the result, request a repeat, or investigate further. This is the clinical judgement element of the role.
Laboratories also participate in external quality assurance (EQA) schemes, where they analyse samples of known composition sent by an external body and compare their results against other laboratories. EQA provides an independent check that laboratory methods are performing correctly over time. To understand how results relate to expected ranges, see our guide on reference ranges explained.
Why some samples are delayed or rejected
Common reasons a sample may be rejected or delayed:
- Unlabelled or incorrectly labelled tube — cannot be safely processed
- Haemolysis — red blood cells ruptured during collection; affects potassium, LDH, and other results
- Clotted sample — when the tube required an anticoagulant and the blood clotted before mixing
- Lipaemia — excess fat in the blood causing the sample to appear milky; can interfere with certain measurements
- Insufficient volume — not enough blood to run the requested tests
- Wrong tube type — additive incompatible with the requested test
- Delayed transport — certain analytes degrade with time or temperature
When a sample is rejected, the laboratory notifies the requesting clinician and usually requests a repeat collection. This can delay results, which is why correct collection technique at the point of care matters so much.
When results reach the clinician
Once a biomedical scientist has authorised a result, it is released from the LIMS to the clinician through the electronic patient record system. In most NHS trusts, results appear in the patient’s record within minutes of authorisation for routine tests, or faster for urgent tests. Critically abnormal results — for example, a potassium level at a dangerous threshold — trigger an alert and require a phone call from the laboratory to the clinical team, regardless of the electronic system.
The entire process, from a blood draw to a reported result for a routine biochemistry test, typically takes between two and four hours for in-hospital samples, and may take longer for samples sent from GP practices or community settings. Urgent tests can be turned around much faster, sometimes within 30 to 60 minutes.
References
- Institute of Biomedical Science (IBMS). Sample Journey. ibms.org
- NHS. Blood Tests. nhs.uk
- Clinical and Laboratory Standards Institute (CLSI). Procedures for the Handling and Processing of Blood Specimens for Common Laboratory Tests. CLSI guideline H18.
- Plebani M, Carraro P. Mistakes in a stat laboratory: types and frequency. Clinical Chemistry. 1997;43(8):1348–1351.
- Lippi G, Guidi GC, Mattiuzzi C, Plebani M. Preanalytical variability: the dark side of the moon in laboratory testing. Clinical Chemistry and Laboratory Medicine. 2006;44(4):358–365.